Meniscal Surgery
Meniscal injuries
The function of the meniscus cartilage in the knee is to act as a shock absorber when walking, running, and jumping and to also stabilise the knee joint.
Damage to the meniscus can occur due to injury, wear and tear, or the presence of arthritis in the knees.
Apart from knee pain and difficulty walking, damage generally results in swelling to the knee as well as locking or clicking of the joint.
Damage will not show up on an x-ray. Instead, an MRI scan is sometimes required to confirm the diagnosis, although in many cases a diagnosis can be made from an examination and knowledge of how the injury was caused.
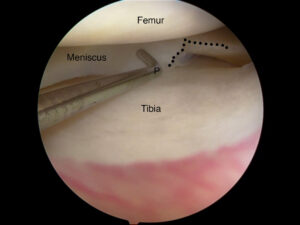
Arthroscopic view of knee with radial meniscal tear.
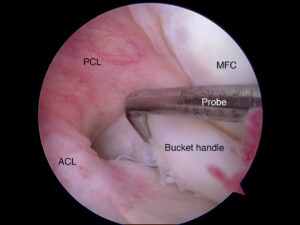
Arthroscopic view of knee with bucket handle tear of meniscus locked in the notch.
Surgery
Meniscal tears often do not heal naturally. The extent and location of the tear will determine which procedure is likely to be more effective.
The meniscus has three zones:
- Outermost Red-Red zone (vascular zone; tears here are likely to heal well with repair).
- Middle Red-White zone (less vascular area; tears may heal in young individuals).
- Inner White-White zone (avascular area, tears unlikely to heal even with repair).
Generally, if the tear is relatively small, a small section of the meniscus can be surgically removed (a ‘partial meniscectomy’). With larger tears to the meniscus, especially in the Red-Red zone, surgery may involve repairing the tear itself with special suture-anchors.
Excision of the meniscal tissue has been proven to be associated with a much higher incidence of degenerative changes/osteoarthritis over the next 10-20 years. There is therefore increasing emphasis to preserve as much meniscal tissue as possible.
Most meniscal surgery is conducted using arthroscopic techniques (keyhole surgery) where two small (about 1cm) incisions are made on either side of the patellar tendon. Meniscal tears associated with ACL (anterior cruciate ligament) tears are often repaired at the time of ligament reconstruction and they have a very high incidence of healing.
Rehabilitation and post-operative care
If the procedure involved removing a section of the meniscus, recovery time is generally three to six weeks and it’s possible to walk bearing full weight of the body straight after surgery. Crutches may be required for pain for 2-5 days after surgery.
However, if the surgery was to repair the meniscus, there is a 4-6 week period after the surgery during which no load bearing is permitted. This aids in meniscal repair healing.
Low impact activities (e.g. general walking and office work) can be undertaken within a week of surgery, however higher-impact activities, such as heavy physical work or playing sports, will require a longer recovery period of around two to six weeks. Dr Sunil Reddy will give you more precise guidelines. Full recovery from a meniscal repair procedure can take up to three months.
Meniscal repair – things you need to know
Recovery
Recovery from arthroscopic knee surgery is much quicker than from conventional open surgery on the knee. Patients are monitored for up to two hours in the recovery room and if all is well are allowed to return home afterwards, with a crutch.
It is recommended that you do not drive immediately after surgery. Please have a friend or relative pick you up.
Dr Reddy will see you on the morning after surgery if an overnight stay is required – commonly after ligament reconstruction procedures. He and the physiotherapist will guide you regarding your exercise regimen.
Patients can walk full weight bearing after a partial meniscectomy, though meniscal repair would require you to be touch-weight bearing only for four weeks.
Total healing time is 12-16 weeks following a meniscal repair and three to six weeks following a partial meniscectomy. Following a partial meniscectomy, you would be able to walk full weight bearing on the same day as surgery and return to sedentary work as early as five to seven days – but heavy manual work may need two to three weeks. Twisting and pivoting is prohibited for six to eight weeks. Driving of automatic-gear car would be possible 2-5 days after knee arthroscopy depending on pain and restoration of strength and balance.
It is normal for the area around the knee to have some swelling and pain for two to three weeks. Pain medication will be prescribed. Keeping the leg elevated and using ice packs on the knee will help reduce swelling.
Risks of surgery
As with any surgery, arthroscopic knee surgery carries the possibility of complications. These include but aren’t limited to:
- Nerve and/or blood vessel damage.
- Numbing and loss of feeling.
- Ongoing pain in the foot or calf.
Most of these complications are very unusual and knee arthroscopy is overall a safe procedure. When performed for correct indications, the benefits far outweigh the risks.
Failure of meniscal repair is a known complication and may cause pain and clicking. This would require a repeat arthroscopy and partial meniscectomy.
Rehabilitation guidelines following meniscal repair
First two weeks
- Straight leg raises.
- Quadriceps and gluteal sets
- Range of movement exercises of knee sitting on a chair.
- Core-strengthening and upper body exercises.
- No resistance exercises.
- No pivoting, twisting, or cutting movements.
- Touch weight bearing only with crutches.
Two to four weeks
- Continue with quadriceps and range of movement exercises.
- Start proprioception exercises.
- Progress with core-strengthening exercises.
- Touch weight bearing only with crutches.
After four weeks
- Proceed to full weight bearing.
- Progress with range of movement, proprioception, and core-strengthening exercises.
- Start resistance exercises only after six weeks – closed chain exercises only until 12 weeks.
- Start slow walking on treadmill and incorporate functional exercises.
- Running after 12 weeks only based on functional and activity / sports-based testing.