Knee Arthroscopy
Arthroscopy or arthroscopic surgery, is often described as ‘minimally invasive surgery’, or ‘keyhole surgery’.
Knee arthroscopy normally involves the insertion of a small camera through a 5mm – 10mm incision (often referred to as a ‘portal’) in the skin, with up to three further incisions made around the knee to allow other special surgical instruments to be used.
Arthroscopic surgery allows for more rapid recovery after surgery than is possible after conventional open surgery, and scarring is kept to a minimum. The procedure is also generally quicker than conventional ‘open’ surgery with patients able to return home on the day of surgery.
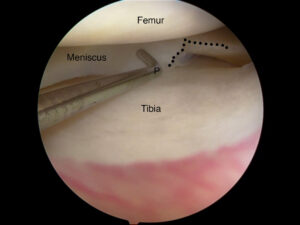
Arthroscopic view of knee showing a meniscal tear.
Knee arthroscopy is generally required for the following procedures:
- For diagnostic purposes.
- To repair or excise torn cartilage/meniscus.
- Clearing infection in the knee joint.
- To correct problems with the kneecap (patello-femoral problems).
- To remove loose pieces of bone or cartilage or to remove cysts in the knee joint.
- Reconstruction of ligaments, especially the Anterior Cruciate Ligament (ACL) and Posterior Cruciate Ligament (PCL).
- Synovectomy – where the joint lining (synovium) is inflamed or pathologic causing effusions, locking, pain, etc.
Procedure
Knee arthroscopy is commonly performed under a general anaesthetic, sometimes in combination with other types of anaesthetic. Spinal anaesthesia, where the patient stays awake during the procedure may sometimes be used. A type of anaesthetic called a ‘femoral nerve block’ may also be used to help block out pain so that a lighter form of general anaesthetic can be used.
Once Dr Reddy has made the incisions as described above, saline or glycine solution is introduced into the knee to allow Dr Reddy to see clearly inside the knee and to operate the arthroscopic instruments. Once the procedure is complete, the saline solution is drained from the knee and the incisions are closed with a single stitch or suture.
Knee arthroscopy – things you need to know
Recovery
Recovery from arthroscopic knee surgery is much quicker than from conventional open surgery on the knee. Patients are monitored for up to two hours in the recovery room and if all is well are allowed to return home afterwards, sometimes with a crutch.
It is recommended that you do not drive immediately after surgery. Please have a friend or relative pick you up.
It is normal for the area around the knee to have some swelling and pain for one or two weeks. Pain medication will be prescribed. Keeping the leg elevated and using ice packs placed on the knee will help reduce swelling.
It may take several weeks to recover completely from arthroscopic knee surgery depending on the procedures performed. Dr Reddy will see you on the morning after surgery if an overnight stay is required – commonly after ligament reconstruction procedures. He and the physiotherapist will guide you regarding your exercise regimen.
Risks of surgery
As with any surgery, arthroscopic knee surgery carries the possibility of complications. These include but aren’t limited to:
- Nerve and/or blood vessel damage.
- Numbing and loss of feeling.
- Ongoing pain in the foot or calf.
Most of these complications are very unusual and knee arthroscopy is overall a safe procedure. When performed for correct indications, the benefits far outweigh the risks.
Rehabilitation guidelines following knee arthroscopy
Timelines mentioned are approximate and progression depends on individual recovery.
Knee arthroscopy does not need intensive physiotherapy postoperatively. Please follow Dr Reddy’s advice regarding exercises.
Apply ice packs three to five times for 10 minutes each time for the first two weeks.
First two weeks
- Static and active quadriceps exercises.
- Straight leg raises.
- Calf presses.
- Hip abduction exercises.
- Core-strengthening exercises.
- Range of movement of knee exercises sitting in a chair.
- Upper body conditioning.
- Progress with gait training to decrease dependence on assistive devices.
Two to six weeks
- Progress with strengthening exercises as tolerated – including squats, hamstring curls, and leg presses.
- Progress with resistance and core-strengthening exercises.
- Start aerobic exercises.
- Emphasise single leg strength, stance, and proprioception.