Total Hip Replacement (THR) is considered one of the most successful treatments in Medicine. 15000 to 20000 THRs are performed in Australia annually. 95% of patients undergoing Total hip replacements have a very good outcome with significant relief in pain and improvement in function. This enables you to return to most activities, work and hobbies you have always wanted to do.
Total hip replacement is an option mainly for people who suffer severe arthritis in the hip. This may be osteoarthritis, i.e. a degenerative condition due to ageing, or inflammatory arthritis.
Total hip replacement is also an option for patients suffering from avascular necrosis, which in turn may be caused by many factors including trauma, alcoholism, steroid use, decompression sickness, etc.
The procedure replaces damaged and diseased cartilage and bone from the existing hip joint and replaces it with an artificial joint. This is made up of two components - the femoral prosthesis which replaces the ball or femoral head, and the acetabular prosthesis which replaces the socket or acetabulum.
Adelaide Orthopaedic Surgeon Dr Sunil Reddy performs Hip, Knee and shoulder replacements using the most up-to-date and evidence–based technologies and implants. He incorporates multi-modality pain relief protocols and blood-loss minimisation measures in all his Arthroplasty procedures to provide the best possible outcome for you.

Representative image of a Total hip replacement.

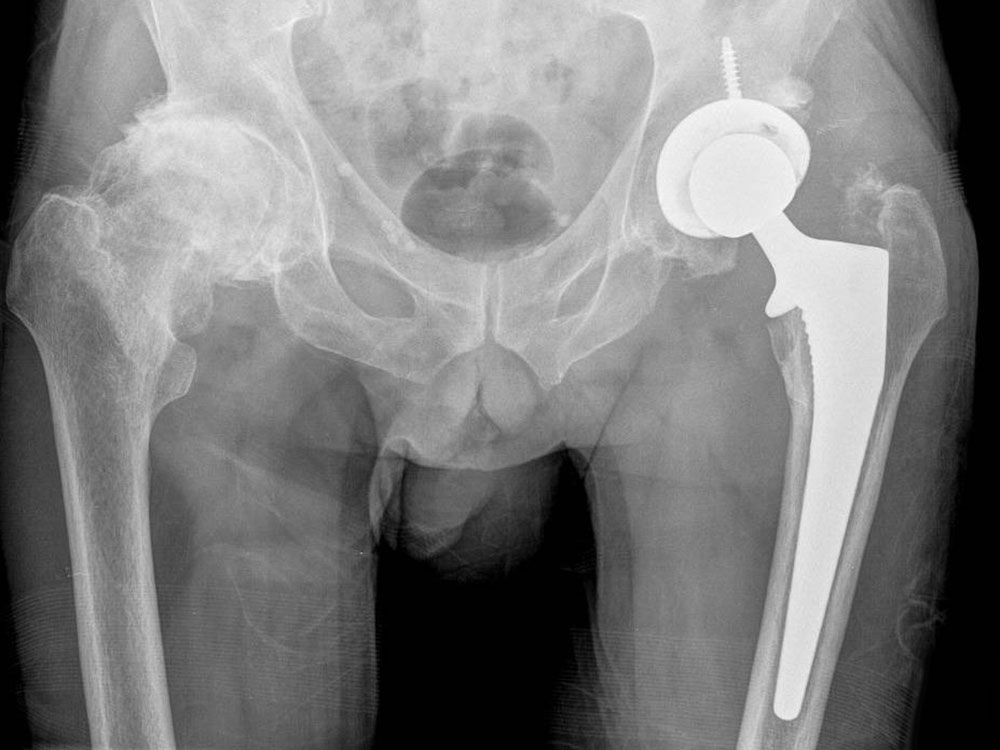
X-ray image of a gentleman with advanced osteoarthritis of both hip joints and after left Total hip replacement.

X-ray image of a hybrid total hip replacement where bone cement is used for femoral component fixation.
Procedure
Total hip replacement is performed under a spinal anaesthetic or under general anaesthesia. A femoral nerve block is administered for pain relief during and up to 48 hours after the surgery.
Dr Reddy as well as your anaesthetist will discuss with you the benefits and risks of the types of anaesthesia and help you decide on the safest and best option.
With the patient lying on his or her side, an incision about 15 cm long is used to expose the hip joint after separating the overlying muscles and ligaments. The socket as well as the upper end of thigh bone(femur) are prepared to allow the artificial joint or prosthesis to be inserted. Dr Reddy uses uncemented implants in most patients younger than 80 years – called Uncemented THR. These implants have a coating on their surface to allow bony integration with the patient’s own socket and femur allowing for a life-long bond. In elderly patients or patients with osteoporosis and poor bone quality Dr Reddy uses special surgical cement to bond the femoral prosthesis to bone. This is called a Hybrid THR.
When the artificial socket is in place, an artificial lining is inserted. In Dr Reddy’s practice this is made of medical grade plastic (High density Poly-ethylene). The new ball may be made of metal or ceramic (has the least amount of wear and suitable for younger people undergoing THR).
The procedure normally takes about 90 minutes.
Direct Anterior Approach Total Hip Replacement (DAA-THR)
Dr Reddy performs Direct Anterior Approach Total Hip Replacement (sometimes known as Anterior Minimally Invasive Total Hip Replacement) routinely in his patients.
Total Hip Replacement – Things you need to know
- A Total hip replacement is a hugely successful procedure. Dr Reddy will discuss with you the benefits, risks and complications of a THR at the initial consult. He will give detailed instructions as to how best to recover from total hip replacement surgery. Your therapist will get you to stand and start exercises as tolerated on the first day. Please follow the advice and perform exercises to give yourself the best chance of recovery.
- The hospital stay is usually 3-4 days, but this depends on individual recovery. Discharge is criterion based rather than days of stay. You can go home once you feel confident and comfortable walking, transferring to chair and managing yourself at home with the help of a friend or family. Sometimes transfer to a rehabilitation facility is required before you gain the strength and confidence to go home.
- Avoid sitting on low chairs, low toilet seats and take precaution when getting in or out of a car, especially for the first 3 months. This is to decrease the risk of dislocation.
- Your hip replacement is stable and strong enough to take loads allowing full weight bearing, walking and activities without any restrictions from day 1. Normal (i.e. not sport or heavy physical) activity can generally be resumed within 3-4 weeks of surgery.
- Patients can resume or take up some sports after a total hip replacement. Sports such as golf, bowls, walking and 'gentle' skiing and doubles tennis are for example perfectly possible. Any sport involving running or contact is not recommended.
- THR is not as physiotherapy intensive as a TKR. Walking regularly and performing exercises as detailed below at home is all that is required in most patients.
Overview of risks
- Infection (about 1 in 150), bleeding, nerve injury resulting in numbness and weakness of leg, blood clots (DVT and Pulmonary embolism) are some of the risks associated with any major hip or knee surgery. Specific risks of THR also include dislocation, limb length discrepancy, fracture of the femur during or after surgery. Early loosening of the implants can occur as a result of failure of bonding with bone or late loosening can occur as a result of poly-ethylene wear and osteolysis. Dr Reddy will discuss with you the benefits, risks and complications of a THR at the initial consult.
Related Topics
Total Hip Replacement (DAA-THR)