Condition
The term 'rotator cuff' describes four muscle-tendon units that connect the upper bone of the arm to the shoulder blade. These muscles merge into tendons and this muscle structure allows the arm to be lifted and rotated. Tears or ruptures of these muscles can be caused by trauma, such as a sports injury, a fall or a motor vehicle accident, but they can also be caused by other factors such as repetitive stress, lack of blood supply or the growth of bone spurs, called 'shoulder impingement'.
Repetitive stress can be work or sports related, with sports such as weightlifting, tennis and rowing and long-term routine movements, such as lifting overhead, often causing the condition.
Decrease in blood supply to these muscles and degeneration of the tendons is also a common cause and this is simply a part of the ageing process, which makes the tendons more prone to tearing (most people have some sort of rotator cuff tear by the age of 80 and more than 50% of people beyond 60 years have tear, which may be asymptomatic).
Tears can be very small or large, and there is seemingly no correlation between the size of the tear and the amount of pain!
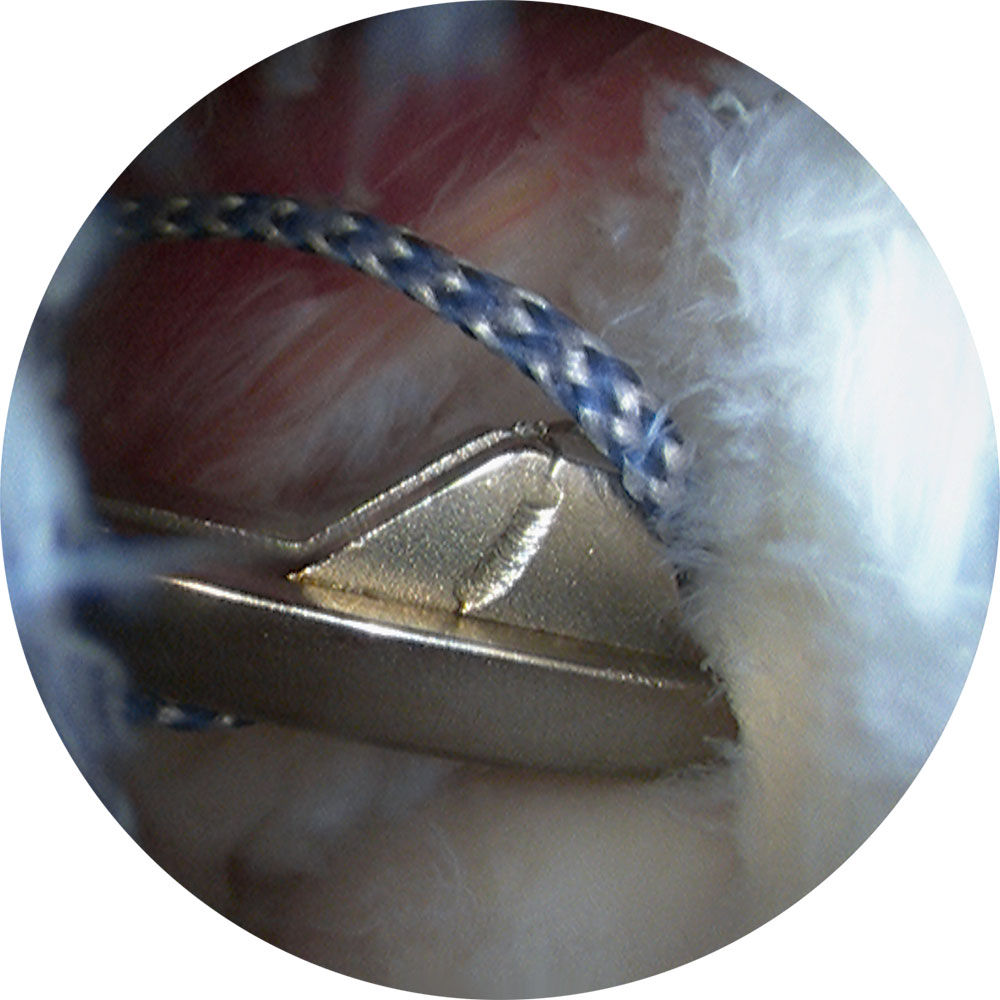
Arthroscopic view of rotator cuff repair.
Procedure
Rotator cuff repair is usually indicated in one of two situations: an acute or acute on chronic traumatic rupture or a chronic symptomatic tear that has failed non-operative treatment.
A rotator cuff repair procedure can be carried out using conventional open surgery or via arthroscopic 'keyhole' surgery or a combination of the two, and is normally performed under general anaesthetic, including an anaesthetic nerve block which helps lessen pain for a 48-hour period.
Adelaide Orthopaedic Surgeon Dr Sunil Reddy specialises in Shoulder and Knee surgery and performs most rotator cuff repairs arthroscopically ( key hole surgery) using the latest evidence-based technologies. This allows for less pain, faster rehabilitation and minimal scarring. He will discuss the benefits, risks and complications of the procedure in detail with you prior to surgery.
Arthroscopic Rotator cuff repair
Arthroscopic or key hole surgery of the shoulder allows for excellent visualisation of the rotator cuff tear and its repair in a minimally invasive manner. It is technically demanding but allows for less pain, early rehabilitation and minimal scars and has equal tendon healing rates as open surgery.
Following arthroscopic evaluation, sub-acromial decompression and management of biceps tendon, the rotator cuff tendon tear or defect is assessed and best repair technique planned. The affected tendons are repaired using small 'rivets' or “anchors” (referred to as suture anchors) which are fixed into the points on the bone where the tendons attach. These anchors are made of PEEK or bio-composite material (that dissolves over a period of time). Over time these connections are strengthened naturally by the body itself.
Dr Reddy repairs most rotator cuff tendons using using a double-row or trans-osseous equivalent technique which allows for a strong repair and in many published studies has shown higher healing rates.
Specific Risks and Complications
Dr Sunil Reddy will explain to you the benefits, risks and complications of this procedure in detail prior to surgery. He will also provide information sheets and encourages you to view the information, videos and rehabilitation protocol on this site.
It is possible that some pain, stiffness and weakness may remain or the repair may fail especially where the tears are larger and where the patient is over 65 or is a smoker, or where the postoperative exercise regime is not followed.
Dr Reddy will demonstrate a self-stretching home exercise regimen that is usually started pre-operatively. This protocol that is continued after surgery has proven to result in excellent shoulder function and range of motion and decrease the incidence of stiffness. If performed correctly, it does not load the rotator cuff during the critical healing period and maintains movement at the same time. Please view and download the attached Shoulder surgery rehabilitation protocol below.
Postoperative recovery and rehabilitation
Dr Reddy as well as the Physiotherapist will see you on day 1 following surgery and demonstrate exercises to be performed at home as well as advise on things to do and not to do.
It is important that you follow the advice and rehabilitation guidelines to give yourself the best chance of recovery and an optimal outcome.
You would likely have a regional / nerve block for pain management apart from a general anaesthetic.
- You would usually stay overnight.
- Please take regular pain medication as advised.
- Apply Ice packs 5 times, for 10 min each time for the first two weeks.
- You will need to wear the sling full time for 6 weeks, but remove it thrice daily for 20 minutes each time to perform exercises.
- Please remove the sling for a shower, resting your arm by the side. The dressings are waterproof.
- After 6 weeks – You can come out of the sling to perform gentle activities of daily living. Progress with exercises as advised by your therapist.
- Strengthening exercises usually start only after 3 months following surgery.
- Avoid lifting weights and push-pull movements for 3 months following surgery. The goal is to gradually achieve normal range of movement and strength of the shoulder over a 3-6 month period.
- Driving is permitted once you come out of the sling and have achieved good control of the arm and a pain-free status. This is usually by the 8-12 week postoperative period.
- Please follow your therapist’s advice regarding exercises and follow the rehabilitation guidelines that you can view / download below.
Download Shoulder surgery rehabilitation protocol (PDF)
Learn more about Rotator cuff tears – Visit American Academy of Orthopaedic Surgeonswebsite.
Related Topics
Rehabilitation guidelines for Arthroscopic/Mini-open Rotator cuff repair