Dr Sunil Reddy performs remnant preserving and hamstring attachment preserving ACL reconstruction using single tendon graft.
Having performed single hamstring tendon reconstruction through the Graft-link method previously, he now strongly believes this newer biologic technique (pioneered by French knee surgeon Dr B. Sonnery-Cottet) has the potential to improve healing and reduce failure rates in ACL reconstruction.
Published medical literature suggests that:
- ACL remnant has vasularised stem cells that can improve healing and ligamentisation of the hamstring graft.
- Preserving hamstring attachment has the potential to atleast partially bypass the stages of avascular necrosis and revascularisation that occur with free tendon graft.
Dr Reddy undertook a 12 week Fellowship at the renowned Centre Orthopaedique Santy in Lyon, France to refine his skills in advanced shoulder and knee surgery, including his current technique of ACL reconstruction.
Conditions
The Anterior Cruciate Ligament (ACL) runs through the middle of the knee from front to back, along with the Posterior Cruciate Ligament (PCL). Together they form an 'X' shape crossing over each other (hence the word 'cruciate' which means 'like a cross'). Their main function is to stop the knee from wobbling forwards and backwards and to stop it from twisting too much.
The ACL can be torn or ruptured in a fall with a pivoting injury or a hyperextension injury of the knee. ACL injuries are common in young people (aged from 15-35) and occur most frequently when playing sports, especially sports like soccer, football, basketball and skiing. Females are slightly more prone to ACL injuries than males due to differences in body anatomy and muscle strength.
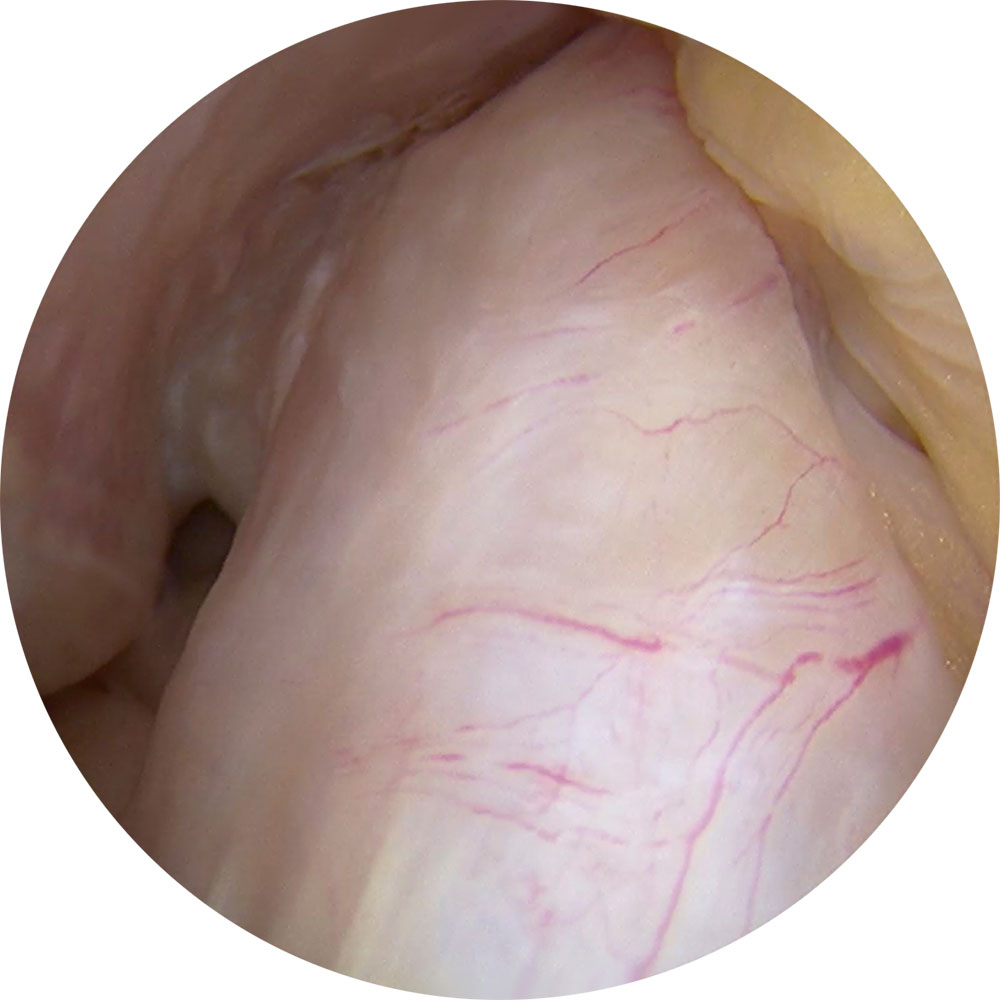
Arthroscopic image of a normal ACL

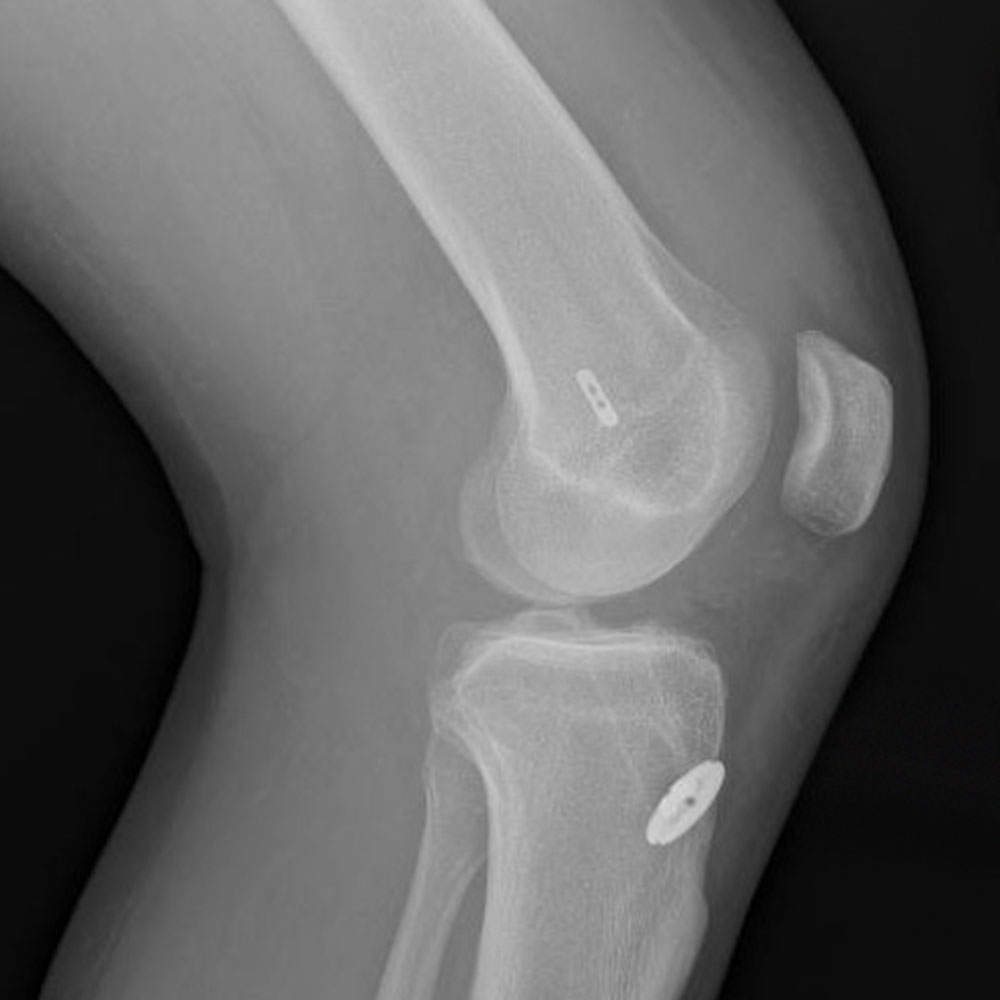
X-ray image of ACL reconstruction with short single hamstring graft with button construct fixation on femur and tibia.
Procedure
Adelaide Orthopaedic Surgeon Dr Sunil P Reddy specialises in knee and shoulder surgery and is experienced in the surgical management of ACL injuries. He practices current evidence-based techniques to provide the best chances for your recovery and return to work or sport.
Dr Reddy performs ACL reconstruction arthroscopically and uses single hamstring tendon (quadrupled or tripled Semi-tendinosus). He occasionally uses patellar tendon graft, especially in revision ACL surgery.
Once the patient is under anaesthesia the knee is examined to confirm that the ACL is torn and to check if there is any damage to other ligaments in the knee.
The graft is harvested through a 3-4 cm incision before ~1cm incisions are made in the front of the knee to allow the arthroscope and other surgical instruments to be inserted. Any damage to the meniscus is addressed before preparing femoral and tibial tunnels for graft fixation.
The surgery usually involves an overnight stay but can sometimes be performed as day-surgery.
Arthroscopic ACL reconstruction – Things you need to know
- Dr Reddy will see you the morning after surgery. He and the physiotherapist will advise you the exercise regimen as well as things to do and not to do. Please follow the advice and regularly perform exercises as detailed below.
- You can walk full weight-bearing after surgery once quadriceps strength and leg control are regained. A pair of crutches is required for the first 1-2 weeks. Twisting/Pivoting and cutting movements as well as high level activity should be strictly avoided for 6 months.
- It is normal for the area around the knee to have some swelling and pain for 2-3 weeks. Pain medication will be prescribed. Keeping the leg elevated and using ice packs placed on the knee will help reduce swelling.
- The dressings are waterproof and showering is allowed.
- Driving is not allowed till complete pain relief and full control of the involved leg is attained. This is usually after 4-6 weeks for the right knee, but may be as short as 2-3 weeks for the left knee with an automatic car.
- The healing and graft maturation following ACL reconstructions continues till the 1-year post-operative period. Return to contact sports is based on functional/sport specific testing and is usually after 9-12 months.
Overview of risks
Risks of knee arthroscopic surgery include nerve injury leading to long term numbness around the knee, bleeding, infection, blood clots (DVT, PE) in the legs or/and lungs. Specific risks of ACL surgery include failure of the graft requiring reoperation, persistent pain in the front of knee, joint stiffness, problems with screws that may be used to fix the graft. Most patients have an uneventful recovery and progress to full healing with a stable knee.
Rehabilitation guidelines for Arthroscopic ACL reconstruction
- The time-lines mentioned are approximate and actual progression depends on individual recovery.
- Patients can weight bear as tolerated from day 1. Please use crutches till good pain control, quadriceps strength and walking mechanics are achieved.
- Avoid pillow under knees and focus on knee extension and quadriceps exercises from day 1.
- Apply Ice packs 3-5 times, for 10 min each time for the first two weeks.
First 2 weeks
- Seated knee range of motion (ROM) exercises.
- Quadriceps sets, hip abductor exercises, core strengthening and upper body conditioning exercises.
- Static quadriceps exercise is the single most important exercise in the first 4 weeks following surgery and you are encouraged to perform it in sets of 20-25, five times daily.
- Gait training. Wean off assistive walking devices.
2-6 weeks
- Closed chain exercises – Start squats, bridge exercise.
- Progress with core strengthening.
- Stationary bike.
- Functional and activity-based exercises.
6-12 weeks
- Add eccentric exercises, lateral training exercises.
- Bike with minimal resistance.
- No cutting, pivoting.
After 12 weeks
- Progress with strengthening and endurance training.
- Low level jumping exercises.
- Work specific and sport specific training.
Related Topics
Rehabilitation guidelines for Arthroscopic ACL reconstruction